ALS (amyotrophic lateral sclerosis) is a progressive disease characterized by muscle weakness due to damage in motor nerves stimulating the muscles. The exact cause of ALS remains to be unknown. However, it is believed that the risk of ALS development is increased by genetic factors, exposure to environmental toxins, smoking, and various chemical substances damaging the cells. ALS usually manifests with weakness in arm and legs muscles or difficulty with speaking and swallowing. Muscle weakness affects daily life, possibly even to the extent of not being able to carry out the simple tasks. Speaking and swallowing becomes even more difficult over time. Respiratory insufficiency which may even lead to death may occur because of the affected respiratory muscles. There is no definitive treatment for ALS disease. A drug named riluzole is used to slow down the progression. Studies on the definitive treatment for the disease and other treatment methods are ongoing.
Table of Contents
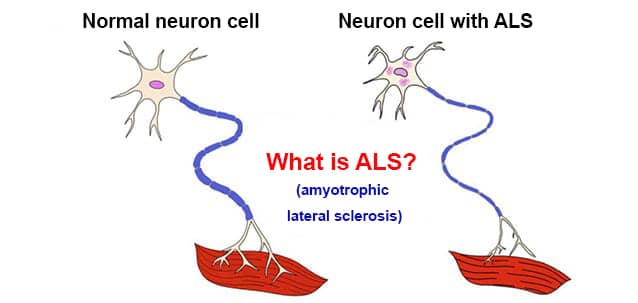
What is ALS?
ALS (amyotrophic lateral sclerosis) is a medical term expressing the muscle wasting and spinal cord damage. Muscles need to contract voluntarily to make a particular body movement. Two groups of nerves called motor nerves work for muscle contraction. When we want to make a movement, a stimulus originating from the involved part of our brain is transmitted to the spinal cord by the first group of motor nerves. Another group of motor nerves in the spinal cord goes from the spinal cord to the related muscle to make it contract.
ALS is a progressive disease due to the damage in upper and lower motor nerves connecting the brain and the muscles, where stimuli cannot be transmitted to the muscle, voluntary muscle contraction gets impaired, and the patient loses their strength partially or completely. Its prevalence is 1-3 in 100,000 individuals.
Approximately 90% of the cases are sporadic, and the remaining 10% are familial. It is slightly more frequent in men. The age of onset of clinical signs is usually 50 to 60. However, it can also be seen at very young or very advanced ages.
Causes of ALS
Certain risk factors for ALS are defined:
Genetic: While more than 130 genetic changes were detected in ALS patients, the most common change was the impairment in the structure of the gene coding superoxide dismutase (SOD) enzyme on chromosome 21.
Excessive glutamate: ‘Glutamate’ which has an important role in the neuronal transmission in the brain has been detected to be at higher levels in patients with ALS: Excessive glutamate damages the neurons.
Impaired cellular metabolism: Each cell has transportation systems which bring the chemical substances into cell and remove the wastes. The impairment of these waste transportation systems in motor neuron diseases disturbs the neuronal functions.
Oxidative stress: Various oxygen species released during cellular metabolism damage the intracellular structures, and cause cellular injury and death.
Amyotrophic lateral sclerosis (ALS)
Autoimmune causes: Neuron death may be seen due to attack of an individual’s immune system to his own neurons.
Age: The risk of getting the disease increases with age. It is most commonly seen between the ages of 40 and 60.
Sex: It is more frequent in men than women.
Environmental factors: Various factors such as smoking; exposure to heavy metals such as lead, mercury, aluminum; infection; exposure to electromagnetic field and head trauma are believed to be associated with the disease. However, no clear evidence has been found, and the mechanism of action is yet to be explained.
Symptoms of ALS
Weakness in all muscles, mainly in arm and leg muscles
Walking difficulty, tottering, and falling.
Difficulty with carrying out the usual daily tasks (difficulty with holding a pencil, difficulty with carrying a glass, and difficulty with buttoning, etc.)
Speaking difficulty
Difficulty with chewing and swallowing
Breathing difficulty
Muscle cramps
Muscular fasciculations
Decreased muscle tone (stiffness)
Uncontrollable laughter or crying
Fatigue, malaise
Starting symptoms are not the same in every patient. Usually, the first symptom to be noticed by the patient is weakness and thinning in one arm or leg. Some patients manifest with speaking or swallowing difficulty.
Breathing difficulty due to involvement of the respiratory muscles
Fatigue due to muscle weakness
Decreased eating and weight loss
Difficulty with sleeping due to discomfort caused by muscle cramps
In the early stages of the disease, bladder and bowel functions are not affected, and eye movements are normal. In the advanced stages, urination difficulty, and though very rare, impaired eye movements may be seen. Sensorial disorder is not seen even at the advanced stages of the disease. If these symptoms are more apparent than the other symptoms, other entities should be investigated.
Diagnosis of ALS
ALS diagnosis is made based on a detailed history taking and findings of neurological examination. As the disease may be mixed up with many different muscle and nerve diseases, additional workup is warranted. As there is no definitive treatment for ALS, hints of treatable diseases are carefully examined.
Medical history: The duration of the complaints, risk factors, family history and the presence of additional illnesses are questioned and evaluated.
Physical examination: Individual muscle strength examination is performed. All body muscles including the tongue are assessed for muscle wasting. The presence of muscular fasciculations is checked, and reflex hammer test is performed. The patient’s speaking, breathing and swallowing functions are assessed.
Electromyography (EMG): It records the electrical activity of the nerves controlling the muscle contractions. In neuronal transmission studies, electrodes are placed on the muscle or skin region related with the nerve to be studied, the nerves of the muscle are stimulated by electricity, and the activity is recorded. Furthermore, needles conducting electricity are pricked to the studied muscle, and the examination is performed when the muscle is still and moving. The patients usually find the procedure uncomfortable and painful. Distinctive findings detected in EMG are important for the detection of both ALS and other diseases in differential diagnosis.
Other methods: As ALS might be confused with other illnesses, blood and urine tests, brain, brain stem and spinal cord magnetic resonance imaging (MRI), genetic tests, taking a sample from the cerebrospinal fluid using needle (lumbar puncture), and muscle biopsy can be performed if necessary.
There is no definitive treatment of ALS disease. Studies on medications are vigorously ongoing. Some medications which can slow down the progression are being used. On the other hand, comforting the patient as much as possible, and taking precautions to make the patient sustain his usual life is crucial. Today, there are many options for the rehabilitation of the patients. These are determined based individually on the patient’s needs.
Medications for ALS
Riluzole: Riluzole has been proven to slow down the disease progression, prevent disease-induced additional conditions, and provides longer functioning time for the patient. However, it is not a definitive treatment. Riluzole blocks the secretion of “glutamate” which is detected to be at high levels in ALS patients. Pills at the dose of 50 mg are taken twice a day. Possible side effects include nausea, vomiting, dizziness and fatigue. It may cause abnormal liver functions.
Edaravone: The efficacy of this medication could not be completely proven in many of the studies on it. It is actively used in Japan and the US. It is used via intravenous route. Its side effects include bruising and allergy.
Other treatments: As many factors are involved in the development of ALS, studies on many medications to find a definitive treatment are ongoing. Moreover, research on gene therapies and stem cell therapies are also ongoing.
Respiratory functions are normal at the early stages of ALS; however, shortness of breath is seen when the disease progresses and affects respiratory muscles. This complaint is seen only during physical activity at first, however later on, it is even seen at lying and sitting position. Continuous positive airway pressure devices can be used.
In patients with worsening respiratory complaints despite using these devices, a hole is opened from the neck into your windpipe (tracheostomy) and a tube is placed into the windpipe. Thereby, respiration can be sustained artificially by means of a device called ventilator. The patient is trained to do breathing exercises. In patients presenting with breathing problems, caution should be taken to avoid infections.
Physical therapy
As weakness is the most common symptom in ALS, exercises are important. Active and passive exercises should be done daily, and position should be changed frequently. To improve the cramps and pain due to immobility, medical therapy is also used in addition to exercises. Pain-killers such as non-steroidal anti-inflammatory medications, gabapentin and opiate can be used for pain; and myorelaxants for cramps.
ALS patients may have difficulties with communication due to speech and breathing problems. Speech therapy may be useful in such cases. Moreover, voice amplifiers can be used to improve decreased voice. Patients who are able to hold a pen can communicate using paper and pencil, or keyboard with the help of adaptive devices.
Swallowing and nutritional support
Swallowing difficulty is caused by restricted jaw and tongue movements, and affected swallowing reflex. Swallowing difficulty gradually worsens over the progression of the disease. In case of solid and liquid foods get into the windpipe, respiratory distress occurs. This risk can be mitigated by adjusting the content, composition and consistency of the foods and beverages. If the patient has abnormal weight loss and respiratory distress due to nutrition problems, gastrostomy procedure can be performed.
Development of nutritional deficiency due to swallowing difficulty impairs the quality of life. The patients should consume a high-calorie diet rich in protein. The proper diet should be arranged by determining the patient’s needs such as calorie, fluid, vitamins, etc.
Psychological support
The patients frequently experience problems such as depression and anxiety. Moreover, uncontrollable laughter or crying episodes may occur. Antidepressants may be used for all these.
While there is no definitive treatment for amyotrophic lateral sclerosis disease, there is not an herbal treatment method either. However, patients try various herbal remedies with the hopes of healing. This is also continuously investigated by researchers.
One of the factors in ALS development is free oxygen radicals. Therefore, more emphasis is laid on the foods with antioxidant properties. To that end, foods containing Vitamin A, Vitamin C, Vitamin E with antioxidant properties, green-leafy vegetables, green tea, and carrots can be consumed.
Breathing problems: Affected respiratory muscles lead to shortness of breath, excessive sputum production and respiratory tract infections. Mortality in ALS patients is most frequently due to respiratory failure.
Speech problems: Most ALS patients develop speech problems over time. While simple pronunciation problems occur at first, they worsen and become difficult to understand over time. Therefore, ALS patients are forced to use various speech aids for communication.
Nutritional problems: Swallowing becomes difficult due to affected swallowing muscles. Weight loss and fluid loss may occur. If the foods go into windpipe due to difficulty with swallowing of solid and liquid foods, lung infections may occur. Thus, tube placement from nose to the stomach or opening a hole from the stomach to the skin (gastrostomy) might be necessary.
Sleeping problems: ALS patients experience sleeping problems due to depression, anxiety, swallowing difficulty, shortness of breath, difficulty with changing body positions due to muscle weakness, and muscle cramps and fasciculations.
Psychological problems: Depression and despair is frequent in ALS patients. Antidepressant medications such as amitriptyline might be necessary.
Dementia: Dementia might be seen in 10% of the patients. It causes memory problems and difficulty with decision making.
ALS and metabolic diseases
During the investigations for the etiology of ALS disease, changes in energy metabolism were also detected. Starting from this point, research has been performed on the relationship of ALS with diabetes and high cholesterol. Some studies have detected that obesity, high body mass index and high cholesterol levels slow down the progression of ALS disease and mitigate the risk of ALS.
While patients with Type 2 diabetes usually have these characteristics, it is believed that the risk of ALS is decreased in Type 2 diabetes. As in Type 1 diabetes, autoimmune mechanisms are at the forefront like ALS disease, it is believed that the risk of ALS is increased. Many studies have demonstrated that hyperlipidemia is protective against ALS disease and reduces the worsening of the disease. While many studies have performed on all these relationships, a definitive result and the involved mechanisms are yet to be clearly detected. Generalization, therefore, is not possible
Women with ALS
Amyotrophic lateral sclerosis is less frequent in women than men. However, “bulbar ALS” which presents with loss of speech and swallowing functions first is more common in women. ALS is seen at more advanced ages in women. It is believed that this is because of the protective effect of the estrogen in women. There is no difference between women and men in terms of lifespan.
ALS progresses differently in each patient. Weakness usually spreads from its point of onset to the other extremities, tongue and pharyngeal muscles. The patient’s daily life might get restricted due to wasting and weakness in all body muscles. The patient may not be able to function alone. They may not even be able to get out of the bed. Therefore, the patients absolutely need a caregiver. Communication problems may occur due to speech problems. If breathing and nutritional insufficiency occurs, in-hospital medical help and breathing device might be necessary.
How long do ALS patients live?
Following the onset of the complaints, the average life expectancy is 2.5 to 3.5 years. One in 5 patients lives more than 5 years, and 1 in 10 patients lives 10 years.
Stephen Hawking and ALS
The famous physicist Stephen Hawking diagnosed with ALS when he was a university student at the age of 21, and after 55 years of fight against ALS, he passed away at the age of 76. He made history not only with his terrific achievements in physics field but also as the longest-lived ALS patient in the medical literature. While scientists do not know the exact reason for this, they have some guesses. They claim that this long lifespan was affected by the young age of diagnosis, his commitment to life, and being able to use quality equipment.
Recommendations for ALS patients
Learn the possible problems caused by your disease from your doctor and take proper measures. You must follow the recommendations of your doctor.
Try to eat regularly to reduce weight loss. If the patient cannot eat himself, the caregiver should help with this. In case of swallowing difficulty, caution should be taken while giving fluid, and soft and small-sized foods should be prepared.
Be mindful of symptoms like being unable to take deep breaths, coughing and low voice tone as they may indicate respiratory failure. Learn and do respiratory exercises.
In order to avoid pressure ulcers in bedridden patients, the in-bed position should be changed every two hours, and the bed sheets should be dry and stretched.
ALS patients might be unable to perform self-care at the advanced stages. Therefore, caregiver should ensure patient’s hygiene, convenient clothes should be preferred.
Settings to increase patient’s social communication should be prepared. Necessary precautions should be taken and speech aids should be used to avoid blocking patient’s social circle due to communication problem caused by inability to speak.
The patient’s home environment should be made suitable for daily activities.